Tennessee’s TARGET Zero Suicide: Technology Assisted Recovery, Growth, Empowerment, and Treatment (NSSP)
The Tennessee Department of Mental Health and Substance Abuse Services (TDMHSAS) proposes Tennessee TARGET Zero Suicide (TARGET) to reduce suicide attempts/deaths among working-age adults ages 25-64 by developing and implementing cross-system suicide prevention strategies, including rapid and enhanced follow-up for 2,250 unduplicated adults (Yr 1: 1,000; Yrs 2-3: 1,250/yr) and prevention training for 570 providers and stakeholders.
TDMHSAS will develop partnerships with emergency departments and inpatient psychiatric units to refer at-risk adults to TARGET for follow-up care following discharge for a non-fatal suicide attempt or suicide crisis. Centerstone of Tennessee will provide telephone and/or face-to-face follow-up within 24 hours, weekly for the first month, and at 3/6/9/12 months. Follow-up will include risk assessment, development of a crisis management plan with the participant, means reduction counseling, and referrals/linkages to treatment services utilizing best practices Applied Suicide Intervention Skills Training (ASIST), Counseling on Access to Lethal Means, and evidence-based Columbia Suicide Severity Rating Scale (C-SSRS). The Tennessee Suicide Prevention Network will provide suicide prevention trainings for clinical providers (e.g., primary, behavioral, emergency, VA) and adult-serving systems (e.g., corrections, workforce development, human services, military). TARGET will also work to implement a Zero Suicides framework across state departments and health, behavioral health, workplace, military, justice, etc., settings. Outcomes will include reduction in suicide attempts by 30% and suicide deaths by 10%. An existing Advisory Council, comprising suicide attempt/loss survivors and other stakeholders, will support TARGET’s goals/objectives: (1) improve care transition/ coordination of at-risk adults post discharge, (2) increase the number of providers and stakeholders trained in adult suicide prevention, assessment, and treatment, (3) increase risk identification, referral, and behavioral health services utilization, and (4) implement Goals 8 and 9 of the 2012 National Suicide Prevention Strategy. Evaluation will be conducted by staff experienced in suicide prevention, and all required reports on outcomes and infrastructure development will be met.
Suicide Deaths by Drug Poisoning, 2023
Data Table:

Source: CDC, 2023
Citation:
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]) Available from URL: www.wisqars.cdc.gov
Injury Outcome: Fatal
Injury Type: All Injury
Data Years: 2023
Geography: United States
Intent: Suicide
Mechanism: All Injury
Age: All Ages
Sexes: All Sexes
Race: All Races
Ethnicity: All Ethnicities
Metro/Non-Metro Indicator: None Selected
YPLL Age: 65
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
MCD – ICD-10 Codes: T40.1 (Heroin); T40.0, T40.2, T40.3 (Opium, Methadone, Other opioids); T40.4 (Other synthetic narcotics); T40.5 (Cocaine), T42.4 (Benzodiazepines); T43.6 (Psychostimulants with abuse potential) AND X60-X84 (Intentional sel-harm)
Year/Month: 2023
Group By: Year
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among People of More Than One Race in the U.S. by Age, 2019-2023
Data Table:
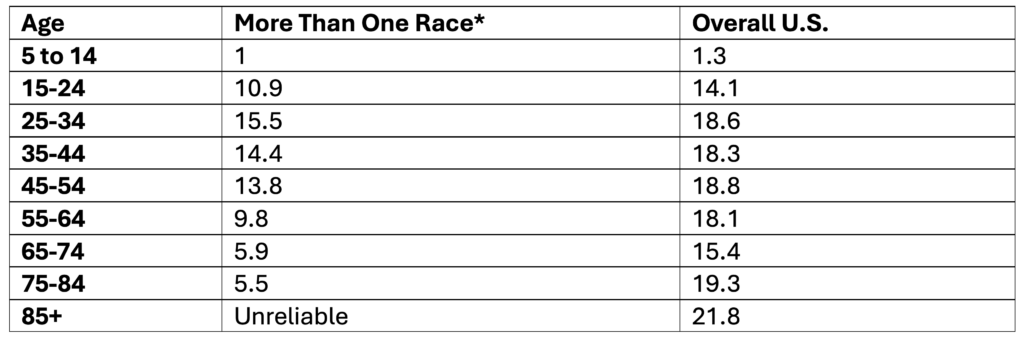
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among White People in the U.S. by Age, 2019-2023
Data Table:
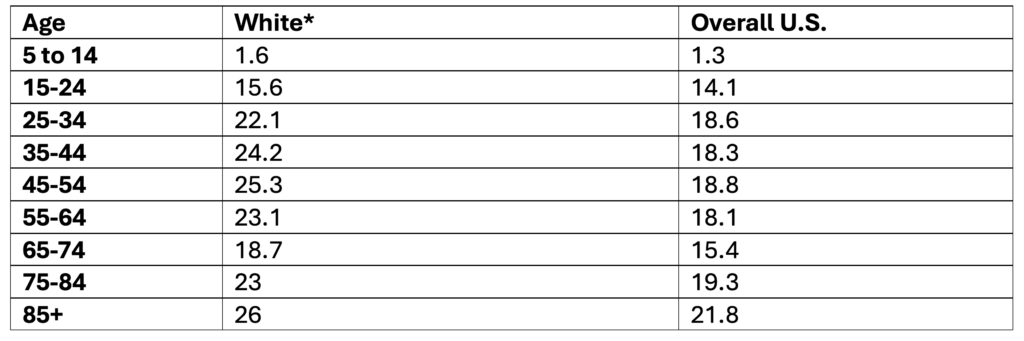
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Native Hawaiian or Other Pacific Islander People by Age, 2019-2023
Data Table:
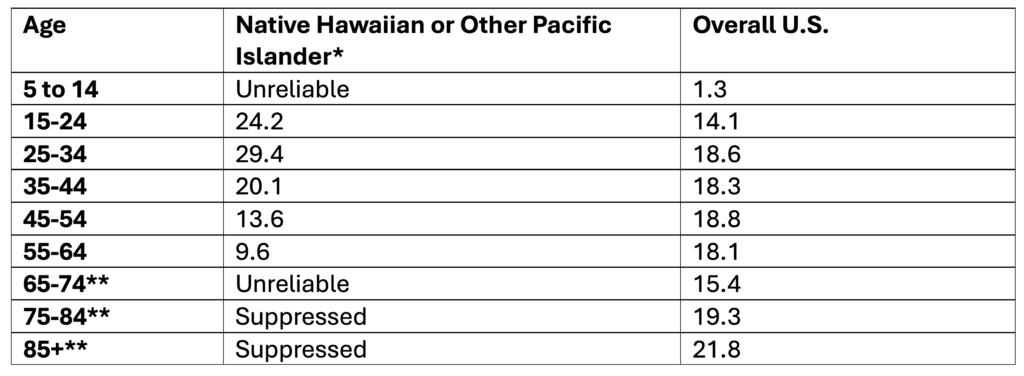
*Non-Hispanic
**Note. Ages 65+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Hispanic or Latino People in the U.S. by Age, 2019-2023
Data Table:
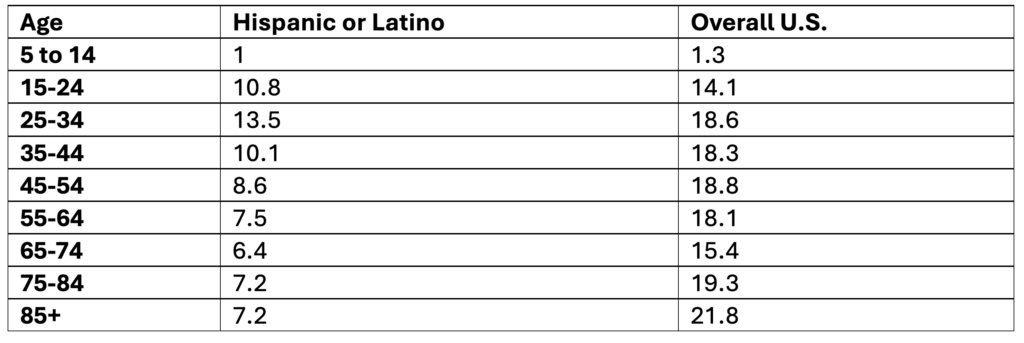
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Hispanic Origin; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Black or African American People by Age, 2019-2023
Data Table:
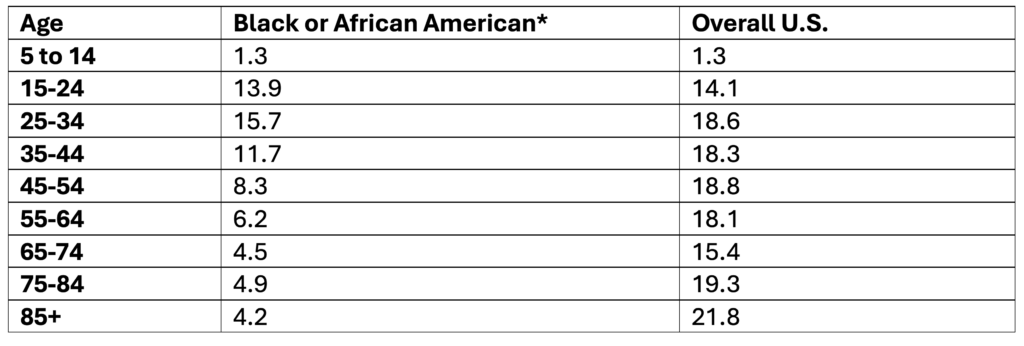
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Asian People in the U.S. by Age, 2019-2023
Data Table:
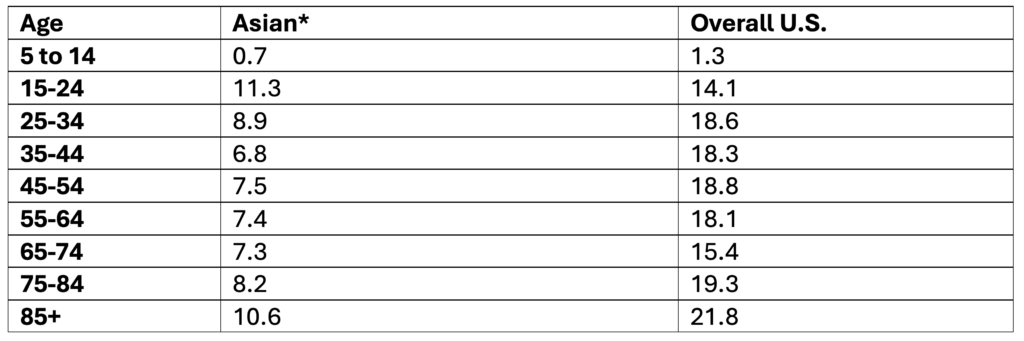
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among American Indian and Alaska Native People by Age, 2019-2023
Data Table:
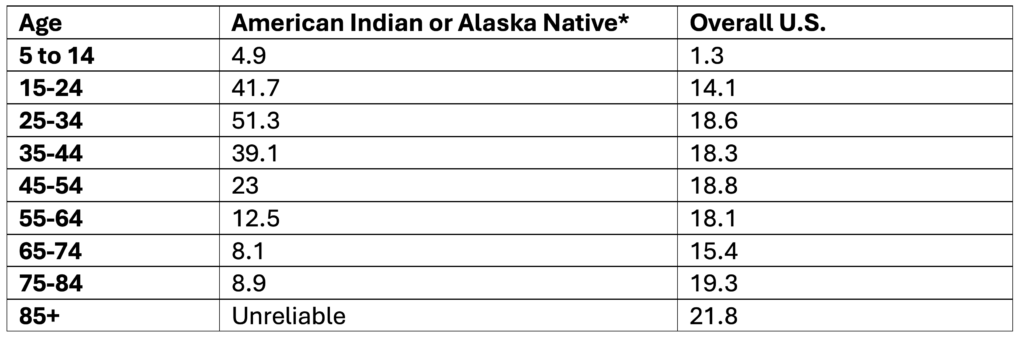
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Past-Year Suicidal Thoughts and Behaviors Among High School Youth, 2023
Data Table:
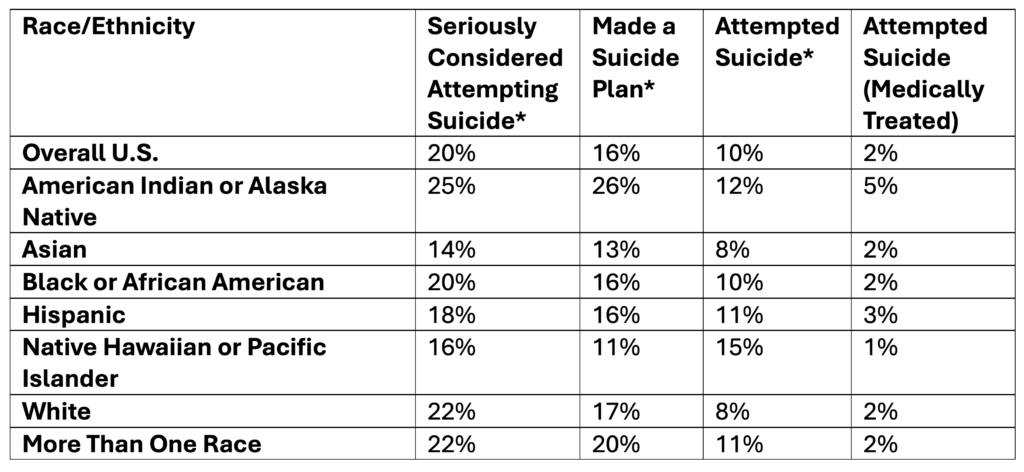
*Self-Reported
Source: CDC, 2025
Citation:
Centers for Disease Control and Prevention (CDC). (2025). 1991-2023 High School Youth Risk Behavior Survey Data. Available at http://yrbs-explorer.services.cdc.gov/.
Past-Year Self-Reported Suicidal Thoughts and Suicide Attempts Among Adults, 2024
Data Table:
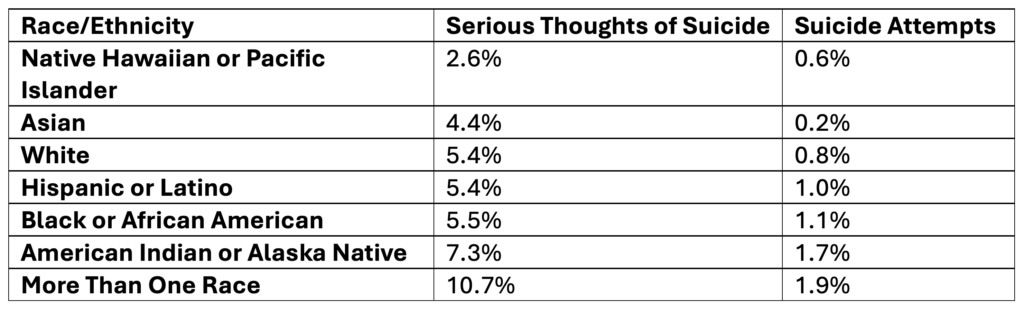
Source: SAMHSA, 2025
Citation:
U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (2025). National Survey on Drug Use and Health 2024 (NSDUH-2024-DS001). Retrieved from https://www.samhsa.gov/data/
Tables: 6.71B & 6.73B
Rates of Suicide by Race/Ethnicity, 2019-2023
Data Table:
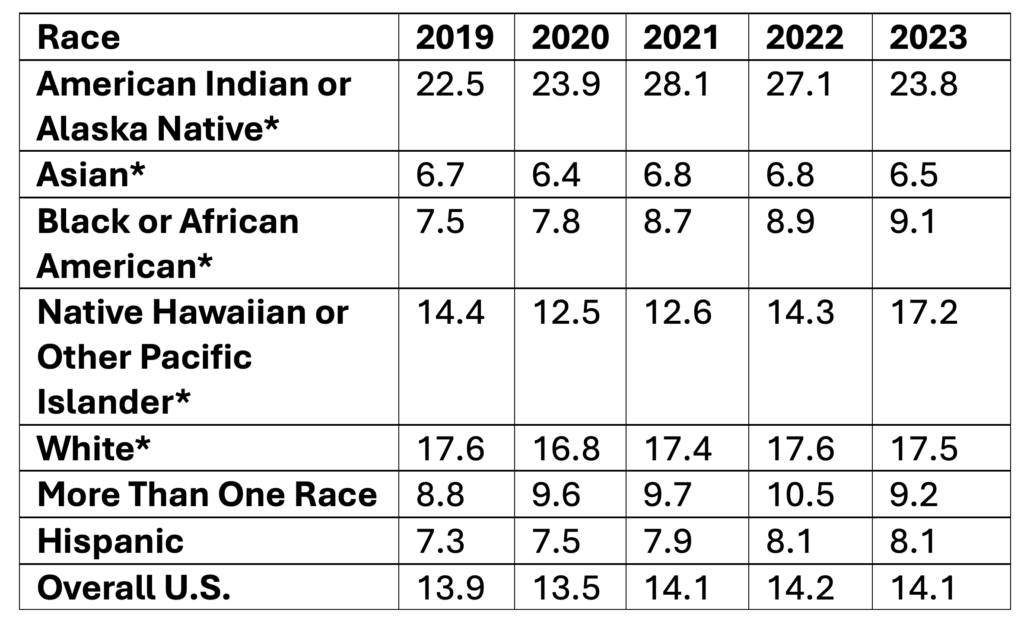
*Non-Hispanic
Age-adjusted rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Single Race 6
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Hispanic Origin
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates by Age, 2019-2023
Data Table:
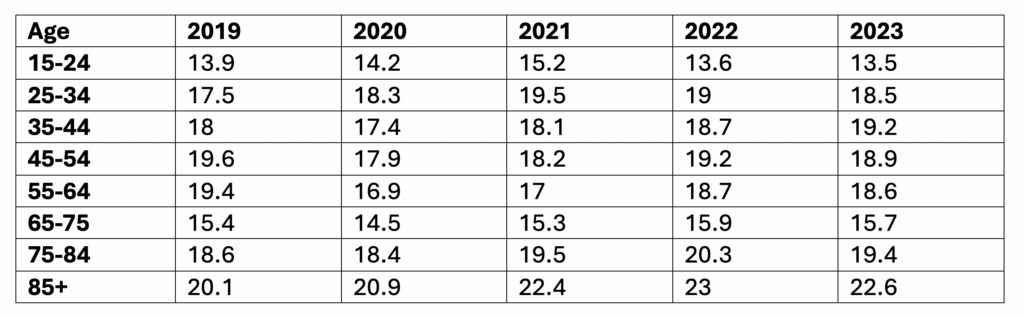
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year, Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)