Pennsylvania Office of Mental Health and Substance Abuse Services
The Institute of Medicine’s the National Strategy for Suicide Prevention (U.S. DHHS, 2001a) clearly identified primary care as a potential source for identification, triage, and brief treatment for suicidal youth. Youth Suicide Prevention in Primary Care (YSP-PC) will build on the success of our current SAMHSA State/Tribal Youth Suicide Prevention Grant by expanding our reach from three counties in northeastern Pennsylvania to eight additional counties in two new regions of the state (southeast and west), the counties with the greatest number of suicide deaths in the Commonwealth. The project will provide primary care providers with the resources necessary to increase a) provider knowledge and comfort with assessing for suicide risk, b) the identification of youth at increased risk for suicide, and c) the number of youth referred from primary care who successfully engage in behavioral health treatment.
In order to achieve this aim, we have five objectives:
- Create state and county level advisory boards consisting of a broad range of stakeholders.
- Provide meidcal practices with educational materials and training that will improve the PCP’s knowledge, confidence and skills to identify and refer at risk youth.
- Provide PCPs free access to a web-based, patient self-report screening tool to assess for suicide and related risk factors.
- Increase the integration of behavioral health services with medical services.
- Provide clinical training to behavioral health providers who receive referrals and treat those at risk for suicide.
There are a number of cultural factors associated with our proposed efforts. While our first grant focused mostly on Caucasian, on low income, rural practices, the YSP-PC project will expand to work with urban and suburban environments, families from a wider socioeconomic status, and broader range of ethnic groups (e.g., Asian, Hispanic). Each demographic provides its own nuances related to risk that will be addressed by local advisory groups. We are also collaborating closely with Pennsylvania’s Medical Home Program to recruit practices since these PCPs already engage in innovative practice models. We have established a partnership with a medical and behavioral health clinic that specifically treats LGBT youth, a university-based health center, and will explore extending our screening program to both juvenile justice and military families. All of these efforts will occur in primary care settings. Our proposal will expand YSP-PC to at least 30 primary care practices by the third year of the project, enabling us to screen over 7,500 youth annually. As with our previous grant, we will continue to call upon our Advisory Board comprised of public and private entities, including state medical associations, managed care organizations, state government, academic and clinical professionals, as well as survivors of suicide to provide oversight, guidance, credibility, and support to our project.
Suicide Deaths by Drug Poisoning, 2023
Data Table:

Source: CDC, 2023
Citation:
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]) Available from URL: www.wisqars.cdc.gov
Injury Outcome: Fatal
Injury Type: All Injury
Data Years: 2023
Geography: United States
Intent: Suicide
Mechanism: All Injury
Age: All Ages
Sexes: All Sexes
Race: All Races
Ethnicity: All Ethnicities
Metro/Non-Metro Indicator: None Selected
YPLL Age: 65
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
MCD – ICD-10 Codes: T40.1 (Heroin); T40.0, T40.2, T40.3 (Opium, Methadone, Other opioids); T40.4 (Other synthetic narcotics); T40.5 (Cocaine), T42.4 (Benzodiazepines); T43.6 (Psychostimulants with abuse potential) AND X60-X84 (Intentional sel-harm)
Year/Month: 2023
Group By: Year
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among People of More Than One Race in the U.S. by Age, 2019-2023
Data Table:
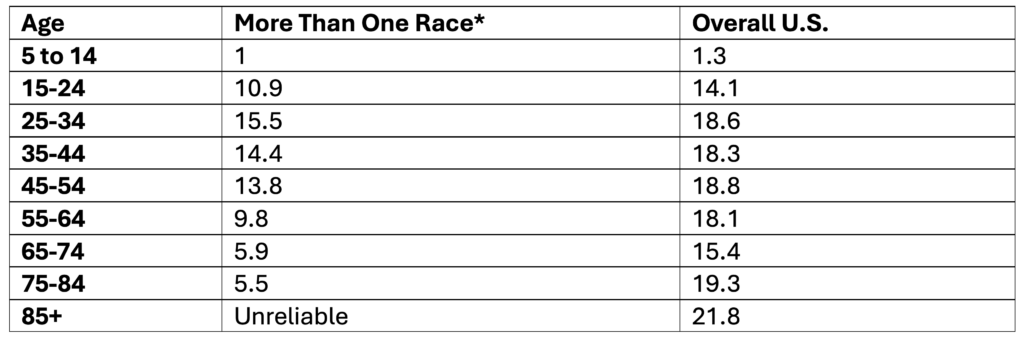
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among White People in the U.S. by Age, 2019-2023
Data Table:
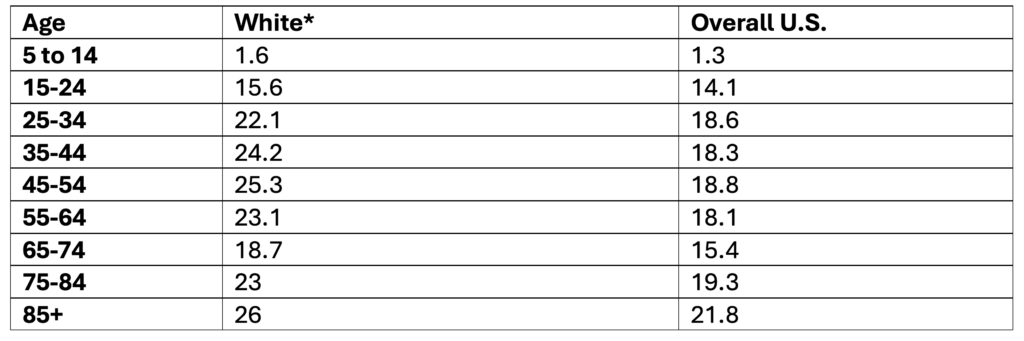
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Native Hawaiian or Other Pacific Islander People by Age, 2019-2023
Data Table:
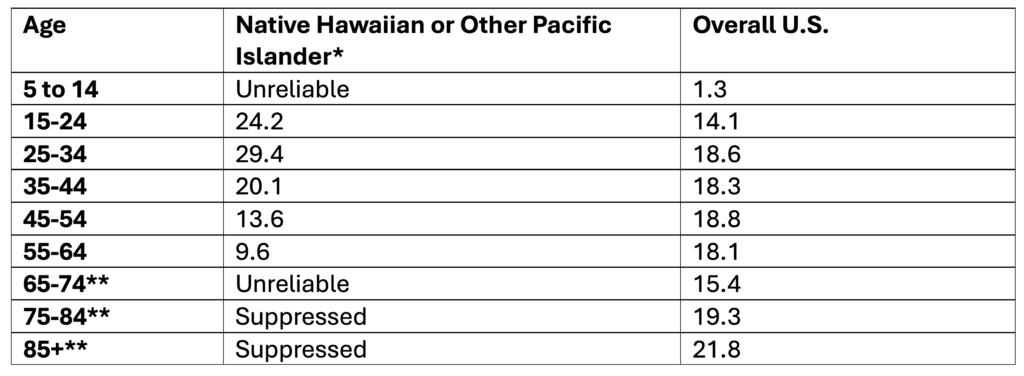
*Non-Hispanic
**Note. Ages 65+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Hispanic or Latino People in the U.S. by Age, 2019-2023
Data Table:
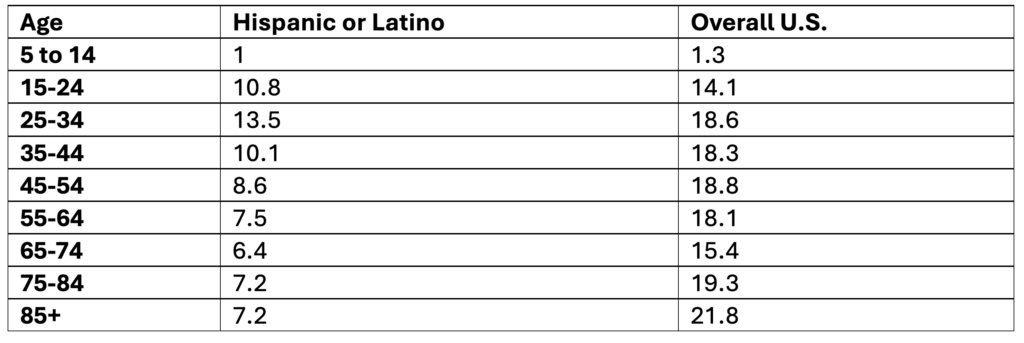
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Hispanic Origin; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Black or African American People by Age, 2019-2023
Data Table:
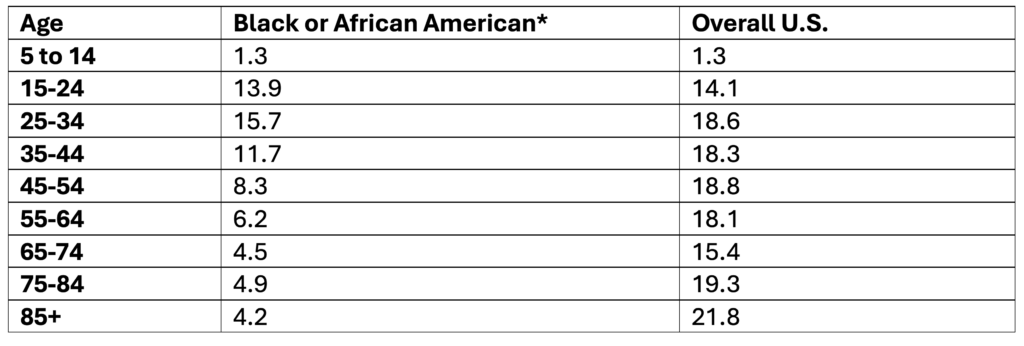
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Asian People in the U.S. by Age, 2019-2023
Data Table:
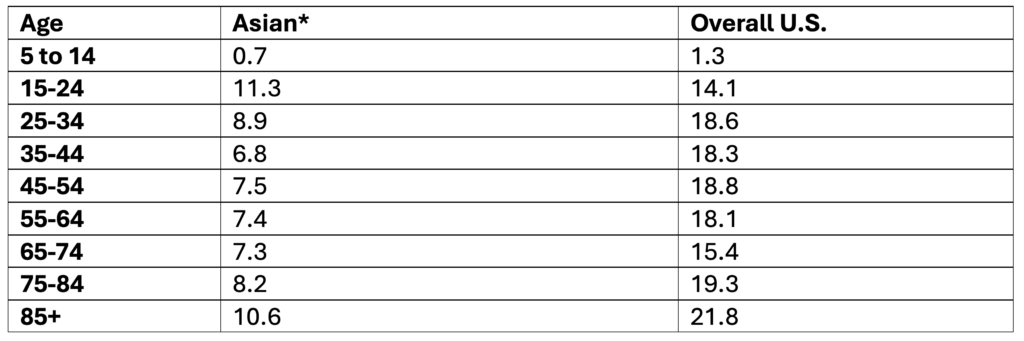
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among American Indian and Alaska Native People by Age, 2019-2023
Data Table:
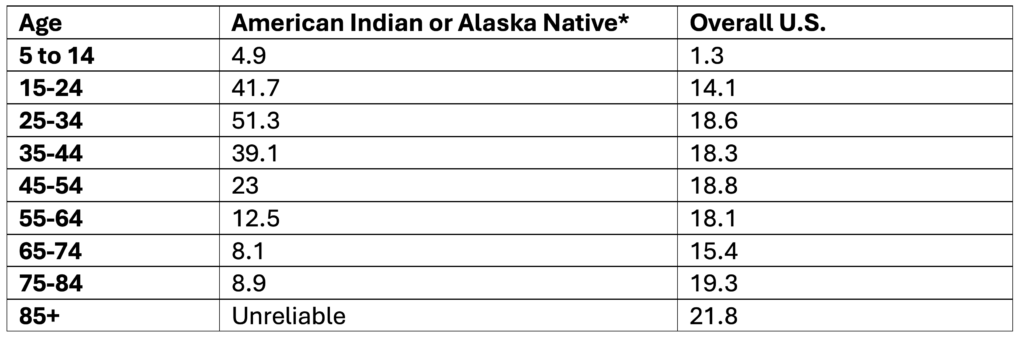
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Past-Year Suicidal Thoughts and Behaviors Among High School Youth, 2023
Data Table:
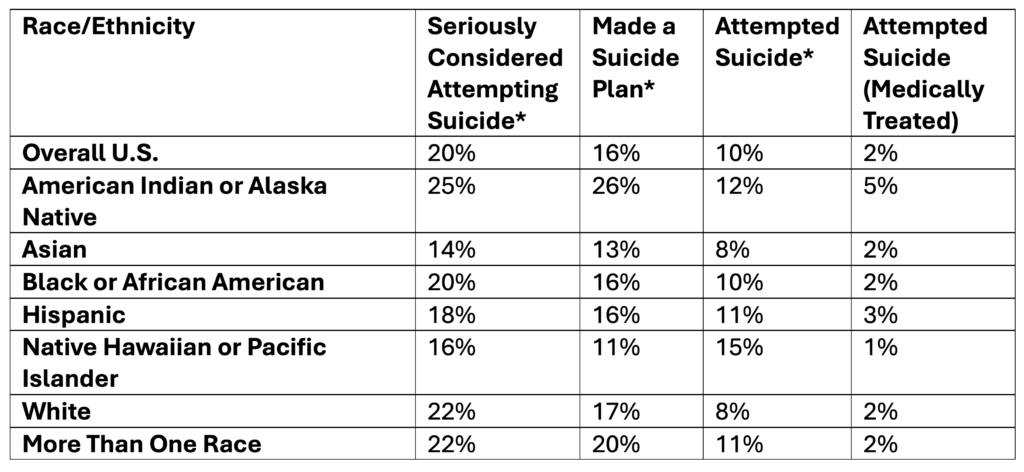
*Self-Reported
Source: CDC, 2025
Citation:
Centers for Disease Control and Prevention (CDC). (2025). 1991-2023 High School Youth Risk Behavior Survey Data. Available at http://yrbs-explorer.services.cdc.gov/.
Past-Year Self-Reported Suicidal Thoughts and Suicide Attempts Among Adults, 2024
Data Table:
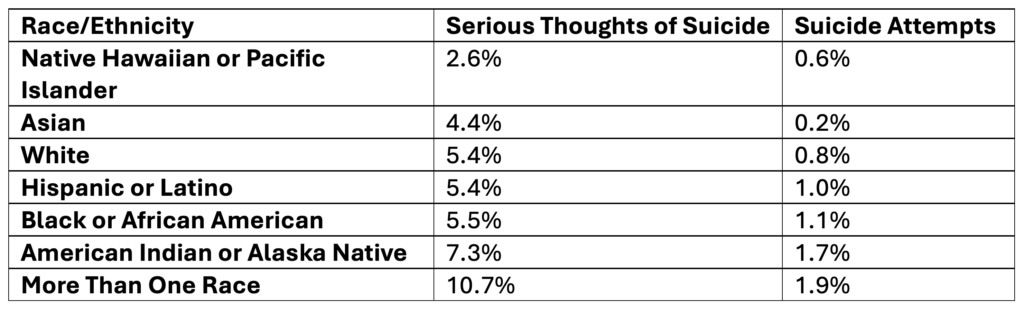
Source: SAMHSA, 2025
Citation:
U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (2025). National Survey on Drug Use and Health 2024 (NSDUH-2024-DS001). Retrieved from https://www.samhsa.gov/data/
Tables: 6.71B & 6.73B
Rates of Suicide by Race/Ethnicity, 2019-2023
Data Table:
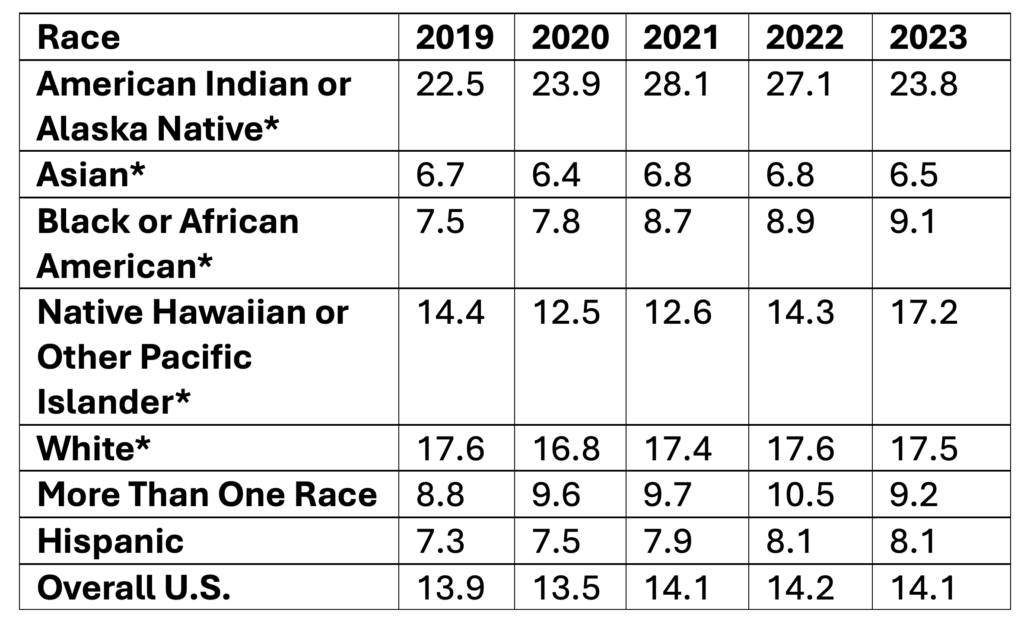
*Non-Hispanic
Age-adjusted rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Single Race 6
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Hispanic Origin
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates by Age, 2019-2023
Data Table:
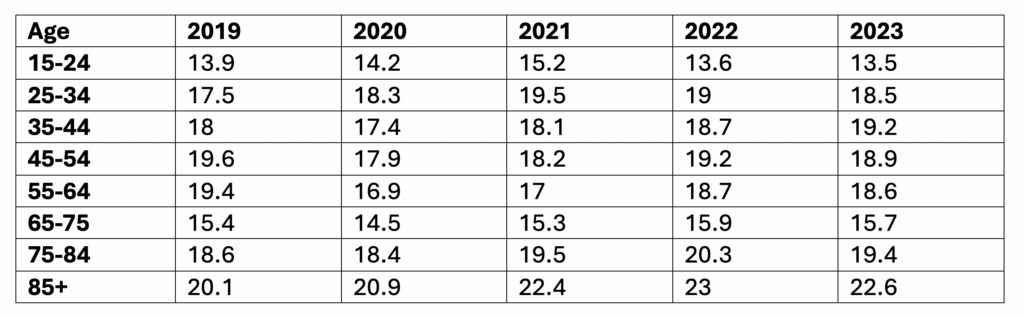
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year, Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)