Clinical Practice Scripts for Suicide Risk Assessment in Clinical Social Work Practice
Introduction
These clinical practice scripts are intended to serve as a bridge between the conceptual framework described in SPRC’s Suicide Risk Assessment and Managing Liability in Social Work Practice issue brief https://sprc.org/wp-content/uploads/suicide-risk-assessment-and-managing-liability-in-social-work-practice.pdf and the recommended resources offered in the accompanying Suicide Risk Assessment Resource Guide https://sprc.org/wp-content/uploads/suicide-risk-assessment-resource-guide.pdf. The four clinical practice scripts in this document were created as a resource for clinical social workers who conduct suicide risk assessments (SRA) with clients. The scripts emphasize the importance of client-centered care and ethical considerations in SRA. In addition to the four clinical practice scripts, this document contains an example of post-assessment documentation.
- Clinical Practice Script 1: Informed Consent and Confidentiality
- Clinical Practice Script 2: Building the Therapeutic Alliance
- Clinical Practice Script 3: Suicide Screening
- Clinical Practice Script 4: Suicide Risk Assessment
- Clinical Note Example: Post-Assessment Documentation and Safety Plan Development
Suggested Citation
Suicide Prevention Resource Center. (2025). Clinical practice scripts for suicide risk assessment in clinical social work practice. https://sprc.org/wp-content/uploads/clinical-practice-scripts-for-suicide-risk-assessment-in-clinical-social-work-practice.pdf
Related Suicide Risk Assessment Documents
- Landing Page (link later)
- Issue Brief: Suicide Risk Assessment and Managing Liability in Social Work Practice (link later)
- Clinical Practice Scripts for Suicide Risk Assessment in Clinical Social Work Practice (link later)
- Suicide Risk Assessment Resource Guide (link later)
Clinical Practice Script 1:
Informed Consent and Confidentiality
Characters and Setting
Jordan is a clinical social worker who provides counseling services at a community mental health center. Alex is an adult client in their mid-20s who is experiencing recent life stress and exhibiting signs of distress. This is Jordan and Alex’s first session together.
Jordan: Hello, Alex. I appreciate you coming in today. It takes courage to come to therapy, and I’m looking forward to working with you. If it’s okay with you, before we start, I’d like to talk about how we’ll work together, what the therapy process looks like, and some other important topics like confidentiality. Is that okay with you?
Alex: Yeah, that’s fine. I’ve never been in therapy before. I went to this support group once, but I wasn’t interested in it. I’m not really sure what to expect.
Jordan: I hear you. People sometimes feel a bit uneasy coming to therapy for the first time, but I’m here to help every step of the way.
So, let’s start by talking about confidentiality. Everything we discuss here is private, but there are some exceptions. If I have concerns that you’re in immediate danger of harming yourself or others, then I may have to share information to help keep you or others safe. I also have to follow legal requirements, like reporting child or elder abuse or complying with a court order. If that ever happens, I’ll explain what’s being shared and why. Do you have any questions about how confidentiality works?
Alex: Thanks for explaining all that. You mentioned one of the exceptions is if a client
is a danger to themselves. Do you mean if I talk about feeling suicidal, you have to report it?
Jordan: That’s a good question. Let me explain a bit further. If a client tells me they are thinking about suicide, I keep that information confidential unless I believe the client is in immediate danger of serious harm. If I think there is immediate danger, I may need to notify my supervisor who can help me to ensure the client’s safety. I would openly communicate with my client about the need for the disclosure, and I would only provide information to my supervisor that is absolutely necessary for keeping my client safe, such as demographic information or information about the client’s concerning behaviors or immediate risk of suicide. Does that answer your question?
Alex: I think so. It’s just a little scary to think about opening up and then having that lead to you telling other people about my private information.
Jordan: I completely understand your concern. Please know that my first step will always be to work with you to ensure that we’re on the same page. I would only break confidentiality if absolutely necessary for your immediate safety. It’s all about supporting your well-being. How does that sound?
Alex: That makes me feel a bit better. I guess it’s good to keep safety in mind like that. But it’s still a lot to take in since I didn’t know exceptions to confidentiality were a thing.
Jordan: Absolutely. This why I discuss this with my clients in our first session. Remember, we are here to talk about your life and work through the concerns you have. I hope you’ll feel comfortable sharing what has been going on so we can work together on your concerns at a pace that feels right for you.
Alex: Okay.
Jordan: Do you have any other questions about anything we’ve covered so far?
Alex: No, it makes sense.
Jordan: Great! One more thing about confidentiality. If I were to run into you in public, let’s say at a grocery store, I’m not able to initiate contact because I would be breaking confidentiality, but you could initiate contact with me if you see me. Does that make sense?
Alex: Yeah, it does.
Jordan: Good! Before we continue, let’s discuss informed consent. This means that before we move forward with assessments or therapy, you have the right to understand what is involved in those things and to decide whether you want to participate. This process keeps everyone on the same page. How does that sound?
Alex: That sounds good to me. Like I said before, this is all new to me. I appreciate you explaining all this.
Jordan: I’m glad to hear that. Now, shall we begin with what brings you in today?
Jordan transitions to asking about the reasons behind Alex’s visit, ensuring Alex feels informed, respected, and in control of their therapy journey.
Clinical Practice Script 2:
Building the Therapeutic Alliance
Characters and Setting:
Jordan is a clinical social worker who provides counseling services at a community mental health center. Alex is an adult client who is experiencing recent life stress and exhibiting
signs of distress. This is their first session together. Jordan has reviewed and completed
the informed consent process with Alex and is now transitioning to focus on engagement
and alliance building.
Jordan: What brings you in today?
Alex: Well, I guess I needed someone to talk to. I’ve just been feeling really down lately. I lost my job a couple of months ago, and it’s been tough to deal with.
Jordan: I’m sorry to hear about your job. That can be a difficult experience. It sounds like it’s had quite an impact on you. Can you tell me a bit more about how you’ve been feeling since this happened?
Alex: It’s like everything I had planned just got turned upside down. I feel lost. The job was everything to me – my routine, my social life, my identity. More and more I just feel empty and worthless.
Jordan: It’s clear that you’re going through some tough times lately. Can you tell me more about the feelings you’ve been having?
Alex: It’s like… I’m in this deep hole and can’t see any way out. I keep thinking if things don’t change, what’s the point? It’s just frustrating and no one seems to understand.
Jordan: It sounds like these thoughts and feelings have been happening pretty often. What are some of the things that can activate these feelings for you?
Alex: It’s mostly when I’m alone at night. That’s when it all hits me – my job loss, my future, just everything. I start thinking that maybe my family and friends would be better off without me.
Jordan: You sometimes feel they would be better off without you. That sounds like a pretty dark place. I’m really glad you’ve recognized this, and you were able to come here today. I am curious, what things, even small things, have kept you going in those tough late-night moments?
Alex: I guess it’s my sister and her daughter, my niece, and, oh, my mom. They mean a lot to me, and we are close as a family, even though I feel like a burden sometimes. I’m not sure how I can climb out at this point, but I’m willing to try. I just don’t want to feel so hopeless all the time.
Jordan: I hear you. We will look into ways to manage these feelings and thoughts, focusing on what gives you a sense of meaning and connection. How does that
sound to you?
Alex: I’m open to trying. I just want to feel like myself again.
Jordan: Remember, you’re not alone in this. I’m glad you chose to come in today. We’ll take this step by step, focusing on what’s important to you and what brings you a sense of hope and purpose.
Clinical Practice Script 3:
Suicide Screening
Characters and Setting
Jordan is a clinical social worker who provides counseling services at a community mental health center. Alex is an adult client who is experiencing recent life stress and exhibiting signs of distress. This is their first session together. Jordan has completed an informed consent process and spent a few minutes engaging and building an alliance with Alex. In the script below, Jordan asks Alex if they have experienced suicidal ideation and introduces the idea of working together to complete a suicide risk assessment.
Jordan: If it’s okay with you, I would like to talk more about the deep hole that you said you feel like you are in. Did these feelings begin around the time you lost your job?
Alex: Yeah, I guess I am fine with talking about it more. . . Yes, it all started around the time I lost my job. I haven’t felt this low in a long time.
Jordan: It sounds like the job loss has had quite an impact on you. Can you tell me a bit more about how you’ve been feeling since this happened?
Alex: After losing my job, I don’t feel like I am the same person. I had so much
hope for my future, and it got wiped out. I feel hollow, like nothing will be the
same after what happened.
Jordan: It sounds like the job was a significant part of your life, not just a means of income but something that gave you a sense of purpose and belonging. Losing something that is important would naturally leave a big void. It’s understandable that you feel a sense of loss, especially considering that your job was very important to you.
Alex: Yeah, and I don’t know how to fill this void. It’s just . . . this all feels pointless. I don’t know what my future will look like now. I go over and over in my mind about where or how to get a new job.
Jordan: Almost anyone in your situation might feel uncertain and overwhelmed when hit by changes like these. Sometimes when people experience a loss or feel overwhelmed, they may have thoughts of suicide. Before our session today, you completed the Patient Health Questionnaire that we ask all our clients to fill out. [Jordan is referring to the PHQ-9.] In your response to the last question, you indicated that you have had “thoughts that you would be better off dead or of hurting yourself in some way” on several days over the past two weeks. And I heard you mention a few minutes ago that you sometimes think your family and friends would be better off without you.
Did I get that right?
Alex [hesitates and looks down]: I didn’t think I would say this, but yes, sometimes I have had those thoughts. It’s like, what if I just didn’t wake up? It feels like that could be an escape from all this mess.
Jordan: Alex, I need to ask you, are you thinking about suicide?
Alex [pauses and hesitates before responding]: Yeah, I have thought about it.
Jordan [calmly]: Ok, thank you for being candid with me. It takes a lot of courage to share these thoughts with another person. You’re taking a significant step by being here and talking about this. What you’re going through is indeed very hard, and it’s understandable that you feel the way you do.
With other clients who have felt this way, I’ve found it helpful to work together to complete a more in-depth assessment. This assessment can help me better understand how things are for you right now and help us figure out ways to keep you safe and help you start feeling better. How do you feel about working on the assessment with me?
Alex: What do you mean by “assessment”?
Jordan: That’s a great question. Completing an assessment means I’ll ask you some specific questions to understand more about what you’re going through, especially regarding your current circumstances and thoughts of suicide. This will help us understand what kind of support you might need to keep you safe. And it will
also help us plan your treatment and get you moving in a positive direction.
Does that make sense?
Alex: So, it’s not a test, right? It’s just talking about what’s going on with me?
Jordan: Exactly. The assessment is not a test with right or wrong answers. We routinely use these assessments in our practice and clients often find that they are helpful. The goal is to help me better understand what is contributing to your thoughts of suicide.
Alex: Ok, I get it. I’m not sure what can help, but I’m willing to try. I just don’t want to feel this way anymore because it is not a good feeling.
Jordan: The fact that you want to feel differently is a great place for us to start. It shows that a part of you is looking for ways to move forward, and we can build on that.
Jordan transitions to completing a collaborative SRA with Alex.
Clinical Practice Script 4:
Suicide Risk Assessment
Characters and Setting:
Jordan is a clinical social worker who provides counseling services at a community mental health center. Alex is an adult client who is experiencing recent life stress and exhibiting signs of distress. This is their first session together. Jordan has completed an informed consent process and spent a few minutes engaging and building an alliance with Alex. Alex received a positive screen on the Patient Health Questionnaire (PHQ-9), so Jordan asked if Alex has been having suicidal thoughts. Alex acknowledged struggling with some suicidal thoughts.
In this script, Jordan transitions into conducting a detailed suicide risk assessment (SRA) using the Columbia-Suicide Severity Rating Scale (C-SSRS) Full Version – Lifetime/Recent, which assesses lifetime and recent history of suicidal ideation and behavior. (There are several versions of the C-SSRS, but in these scripts we’ll use the abbreviation C-SSRS to refer to the C-SSRS Full Version – Lifetime/Recent.)
Jordan begins the conversation by asking Alex the questions about suicidal ideation that appear on the C-SSRS. This script presents the conversation between Jordan and Alex as they complete the C-SSRS. Jordan asks all questions according to the C-SSRS protocol. In addition, Jordan leans into their clinical curiosity by asking other relevant questions to better understand Alex’s history of suicidal thinking.
Columbia-Suicide Severity Rating Scale (C-SSRS) Full Version – Lifetime/Recent assessment: https://cssrs.columbia.edu/documents/lifetimerecent/
Versions of the C-SSRS for use in different healthcare settings: https://cssrs.columbia.edu/the-columbia-scale-c-ssrs/cssrs-for-communities-and-healthcare/#filter=.healthcare.english
Jordan: Alex, given what you’ve shared so far, I think it would be beneficial for us to do an assessment known as the Columbia-Suicide Severity Rating Scale, or C-SSRS. It is a series of questions designed to help us better understand your suicidal thoughts, both in the past month and in your lifetime. If it’s okay with you, we’ll start with the first question. In your lifetime, have you ever wished you were dead or wished you could go to sleep and not wake up? [C-SSRS Suicidal Ideation Question 1 (Lifetime)]
Alex: Yes. I have been feeling that way recently, especially at night when I can’t sleep. It’s been a lot worse since I lost my job. I also had a tough time when I was younger.
Jordan: That must be hard. It can be common for people to feel that way, especially when they are feeling overwhelmed or when something difficult happens, like losing a job. The next question is the same, but it just asks about how you’ve been feeling in the past month. In the past month, have you ever wished you were dead or wished you could go to sleep and not wake up? [C-SSRS Suicidal Ideation Question 1 (Past Month)]
Alex: Yes.
Jordan: Have you actually had any thoughts of killing yourself in your lifetime?
[C-SSRS Suicidal Ideation Question 2 (Lifetime)]
Alex: Yes
Jordan: What about in the past month?
[C-SSRS Suicidal Ideation Question 2 (Past Month)]
Alex: Yes, I have had those thoughts over the last several weeks.
Jordan: In your lifetime, have you thought about how you might do this?
[C-SSRS Suicidal Ideation Question 3 (Lifetime)]
Alex: Yeah . . . I looked up some medications and how people can use them to die.
I tried to kill myself once when I was younger with some pills.
Jordan: Thank you for sharing that with me. That sounds really difficult. Can you tell me more about when that happened?
Alex: I think I was about 15 or 16. It was a bad time, stuff was really hard at home, and I just felt like I couldn’t deal with it anymore.
Jordan: I appreciate you telling me that, it’s important for me to get the whole picture. What about in the past month, have you been thinking about how you might do this?
[C-SSRS Suicidal Ideation Question 3 (Past Month)]
Alex: Yeah. I have.
Jordan: Thank you for answering these questions. I know this isn’t easy to talk about, and I really appreciate your openness. It takes a lot of courage to share something so personal. You’re not alone in this, and I want to work together to figure out how to support you.
Alex: Yeah, it’s been tough. A few weeks ago, I’d had a few beers, and I was struggling to sleep. I held a bottle of Tylenol and wondered what would happen if I just took the whole bottle of pills. I just felt like the world would be better off without me. I felt hopeless. I didn’t do anything though. I just kept drinking and passed out on the couch.
Jordan: Your willingness to share is incredibly important. Can you tell me more about that night?
Alex: I thought about overdosing that night, but I didn’t want to be a burden to my mom. She’s always worried about me and having to clean up after my messes. I don’t want to cause her any more problems.
Jordan: Your concern for your mom speaks volumes about your character. It’s a powerful reminder of how connected you are to those you care about.
[Jordan next asks C-SSRS Suicidal Ideation Questions 4 and 5. We pick up on the conversation when Jordan transitions to the next section of the C-SSRS, which focuses on the intensity of suicidal ideation.]
Jordan: Okay, in your lifetime, when were these thoughts the most severe? Can you tell me, on a scale from 1 to 5, with 1 being the least severe to 5 being the most severe?
[C-SSRS Intensity of Ideation – Item 1 (Most severe, lifetime)]
Alex: It was the most severe when I was a teenager. I would say it was about a 5.I just didn’t see any way out. I felt completely alone and misunderstood.
Jordan: Okay, In the past month, when were these thoughts the most severe? Again, can you tell me on a scale from 1 to 5, with 1 being the least severe to 5 being the most severe? [C-SSRS Intensity of Ideation – Item 1 (Most severe, recent]
Alex: Oh, they were most severe right after I lost my job. So, probably a 4.I felt like I was a ghost of a person. And when I looked in the mirror, I didn’t even recognize myself.
Jordan: How many times have you had these thoughts throughout your life?
[C-SSRS Intensity of Ideation-Frequency (Lifetime)]
Alex: In the time before I tried to overdose when I was 15 or 16, I thought about it every day.
Jordan: What about in the past month? [C-SSRS Intensity of Ideation-Frequency
(Past Month)]
Alex: You mean, how many times have I had these thoughts?
Jordan: Yes.
Alex: Lately, I’ve thought about it a lot more often. I can’t sleep and it reminds me a lot of how it felt when I was a teen. I’ve tried to push the thoughts away.
Jordan: So, you went from a 5 when you were a teenager to a 4 more recently. I’m curious, and this isn’t a question on the form, but what has changed?
Alex: I guess, maturity and knowing myself better.
Jordan: I think one of your strengths is being able to recognize when you’re in distress. So, the next question on the form is, in your lifetime when you’ve had the thoughts, how long did they last? [C-SSRS Intensity of Ideation-Duration (Lifetime)]
Alex: Before I tried to kill myself, I thought it about it all the time. I couldn’t focus on anything else. Lately, I’ve noticed these thoughts come and go throughout the day. Then they get worse at night and that is when I have a harder time controlling them.
Jordan: And in the past month, how long do the thoughts last?
[C-SSRS Intensity of Ideation-Duration (Past month)]
Alex: Most of the day.
Jordan: Can you stop thinking about killing yourself or wanting to die if you want to?
[C-SSRS Intensity of Ideation-Controllability (Lifetime)]
Alex: It depends on what’s going on that day. Mostly I can control it throughout the
day by distracting myself by watching TV. Like I said, the thoughts are harder to
control at night.
Jordan: So, would you say that you can control the thoughts with little difficulty, some difficulty, or a lot of difficulty? [C-SSRS Intensity of Ideation-Controllability (Past month)]
Alex: Um, well, some difficulty.
Jordan: In your lifetime, have there been things – anyone or anything (e.g., family, religion, pain of death) – that stopped you from wanting to die or acting on thoughts of suicide? [C-SSRS Intensity of Ideation-Deterrents (Lifetime)]
Alex: Definitely. My family, especially my sister, my niece, and my mom, are important
to me. When I was a teenager, I didn’t think about how much it would hurt them; I was only focused on myself. It wasn’t until after I overdosed that I understood how much
pain I caused.
Jordan: In the past month, are there things – anyone or anything (e.g., family, religion, pain of death) – that stopped you from wanting to die or acting on thoughts of suicide? [C-SSRS Intensity of Ideation-Deterrents (Past month)]
Alex: Definitely still my family. Also, my dog is my best friend, and she relies on me, so I can’t leave her.
Jordan: And what sorts of reasons would you say you had for thinking about wanting to die or killing yourself, both in your lifetime and in the last month? [C-SSRS Intensity of Ideation-Reasons for Ideation (Lifetime)]
Alex: As a teenager, I would say to end the pain. There was a lot of emotional pain that I was dealing with and still deal with to this day. I wasn’t trying to get back at anybody then. I was just trying to not feel so much.
Jordan: And what sort of reasons would you say you had for thinking about suicide in the last month? [C-SSRS Intensity of Ideation-Reasons for Ideation (Past month)]
Alex: I guess it’s the same now. I just don’t see a purpose for why I’m here and that hurts. You know, if I don’t find work soon, I won’t even be able to buy dog food. So, you know, what am I doing?
Jordan: That’s a very stressful situation to be in, not knowing if you would be able to take care of your dog. Do you need a break, or do you feel comfortable moving forward? I have a few more questions to ask, but if you need a break, we can take one.
Alex: No, I’m okay.
Jordan: I appreciate you sharing that. I want to make sure we come back to this concern about not being able to afford dog food and how it’s impacting you. For now, let’s continue with the questions, but we’ll revisit this later.
[Jordan and Alex complete the rest of the form.]
Jordan proceeds to ask Alex about the dates and actual lethality/medical damage of their previous suicide attempt.
Jordan: Thank you for being so open, Alex. I know this is not an easy assessment to complete, but I now have a better understanding of your situation and what you’ve been dealing with over the last couple of months. Based on our conversation, I think it would be a good idea to explore how we can relieve some of your feelings of hopelessness and ensure your safety. We can also discuss support options. We’ll take this one step at a time, focusing on your well-being.
Jordan proceeds to conduct a safety planning intervention with Alex using the Stanley-Brown Safety Plan. Jordan and Alex work together to develop support strategies, maintaining a collaborative and supportive environment throughout the session.
Clinical Note Example:
Post-Assessment Documentation
and Safety Plan Development
Below is an example of a clinical note documenting Jordan’s first session with Alex, including documentation of the SRA. Some of the details in this example clinical note come from parts the SRA conversation between Jordan and Alex that were not represented in the clinical practice scripts.
Session Overview
Today (Date) marked the initial appointment and first assessment with Alex, who reported recent suicidal ideation. Alex reported recent job loss and feelings of hopelessness and worthlessness. Alex expressed, “It’s like . . . I’m in this deep hole and can’t see any way out,” indicating a significant level of distress. Alex also stated they “sometimes” think about suicide. The session focused on identifying Alex’s reasons for coming to therapy, assessing Alex’s current mental state, understanding the factors contributing to their suicidal ideation, and collaboratively developing a comprehensive safety plan.
Risk Assessment
Alex’s risk of suicide was assessed as moderate. The overall assessment of Alex’s suicide risk as “moderate” was determined through a suicide risk assessment (C-SSRS) that was conducted and completed during this session after Alex disclosed suicidal ideation. In the assessment, key suicide risk indicators for Alex included recent job loss, the presence of defined suicide means (overdose with medications) in the home, one prior suicide attempt, and a clear expression of recent suicidal ideation. Alex denied having the intent to act on their ideation or having a suicide plan. Alex demonstrated a willingness to engage in suicide safety planning and expressed ambivalence about acting on the recent suicidal thoughts, stating, “My family, especially my sister, my niece, and my mom, are important to me.”
Safety Planning Intervention
The suicide risk curve was discussed with Alex and a detailed safety plan (Stanley-Brown Safety Plan) was developed in collaboration with Alex. The plan includes:
Warning Signs: Alex/Client and Jordan/Clinician discussed recognizing early signs of a suicidal crisis, such as overwhelming sadness, isolation behaviors, and increased alcohol consumption. Alex noted, “I felt like I was a ghost of a person. And when I looked in the mirror, I didn’t even recognize myself.“
Internal Coping Strategies: Alex identified several effective coping strategies, such as photography and listening to music. Alex expressed, “Photography used to give me so much joy. I want to start doing it again.”
People/Places That Provide Distraction: Alex identified spending time with family, particularly their niece, as a good distraction from their problems. They also identified taking their dog for a walk as a helpful distraction activity.
People to Ask for Help: Alex listed key individuals to reach out to when feeling vulnerable, namely their sister and a trusted friend. We discussed the importance of having direct conversations with the selected individuals to ensure they are prepared to offer support.
Professionals or Agencies to Contact During a Crisis: Alex committed to calling either this clinician or the 988 Lifeline if a crisis arises before the next session. Alex confirmed, “If things get really bad, I’ll call you, or if you’re not available, the 988 Lifeline.”
Reducing Access to Lethal Means: Alex identified having access to pills as a potential means for suicide. Following discussion, Alex agreed to have their sister pick up the medications for storage outside of the home. Alex stated, “I’m okay with my sister keeping the medications until things get better.” Alex called their sister on speakerphone during the session and confirmed plans to have them assist with securing the medications later that same day.
Engagement in Treatment: Alex agreed to engage in therapy for at least the next three months to address the underlying issues related to their suicidal behaviors. Alex acknowledged, “I need help to get through this, and I’m willing to give therapy a chance for the next few months.”
A copy of the safety plan was given to Alex, and another copy has been uploaded to the Alex’s chart. Jordan discussed with Alex that they would review the safety plan together at their next session to confirm that the strategies listed were useful.
Supervisor Consultation:
Consultation with supervisor was conducted post-session. The supervisor concurred with the assessment of moderate risk and supported the outlined safety plan, affirming its robustness and appropriateness for outpatient care.
Plan:
- Continue weekly sessions focusing on addressing Alex’s feelings of hopelessness and loss of purpose, while reinforcing the use of identified coping strategies.
- Regularly review and update Alex’s safety plan as needed.
- Monitor Alex’s adherence to the safety plan, particularly regarding means restriction and crisis response readiness.
- Explore and work with Alex to address underlying factors (e.g., job loss) contributing
to Alex’s current mental state and collaboratively work on building resilience and
finding purpose.
Clinician’s Observations and Reflections
Alex displayed self-awareness and a willingness to engage in the therapeutic process, which is promising for future sessions. Their openness to creating and adhering to a safety plan suggests a good prognosis for outpatient treatment. Alex stated, “I will do my best to follow this safety plan and promise to call you or 988 if I start experiencing suicidal thoughts.” Ongoing assessment of Alex’s mental state and risk factors will be crucial in our work together.
Suicide Deaths by Drug Poisoning, 2023
Data Table:

Source: CDC, 2023
Citation:
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]) Available from URL: www.wisqars.cdc.gov
Injury Outcome: Fatal
Injury Type: All Injury
Data Years: 2023
Geography: United States
Intent: Suicide
Mechanism: All Injury
Age: All Ages
Sexes: All Sexes
Race: All Races
Ethnicity: All Ethnicities
Metro/Non-Metro Indicator: None Selected
YPLL Age: 65
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
MCD – ICD-10 Codes: T40.1 (Heroin); T40.0, T40.2, T40.3 (Opium, Methadone, Other opioids); T40.4 (Other synthetic narcotics); T40.5 (Cocaine), T42.4 (Benzodiazepines); T43.6 (Psychostimulants with abuse potential) AND X60-X84 (Intentional sel-harm)
Year/Month: 2023
Group By: Year
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among People of More Than One Race in the U.S. by Age, 2019-2023
Data Table:
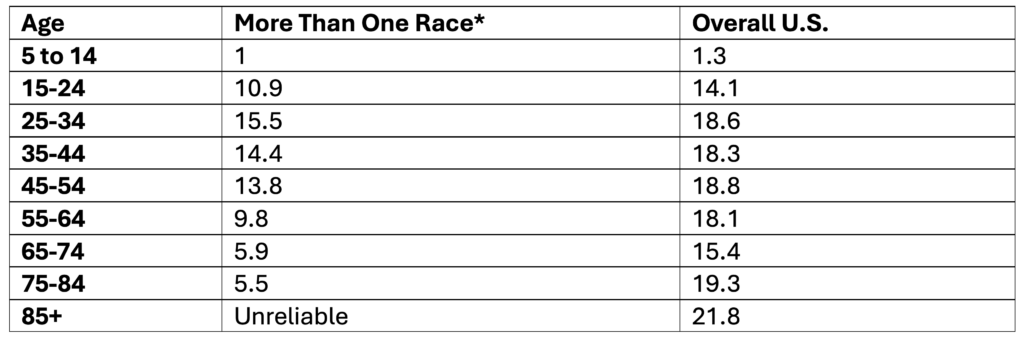
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among White People in the U.S. by Age, 2019-2023
Data Table:
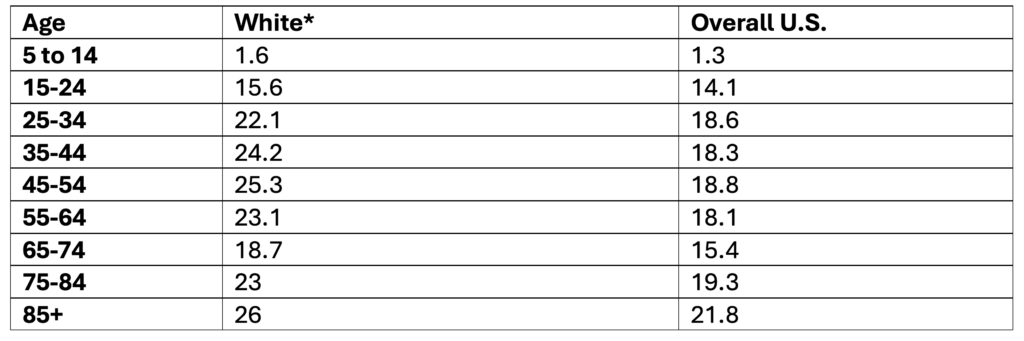
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Native Hawaiian or Other Pacific Islander People by Age, 2019-2023
Data Table:
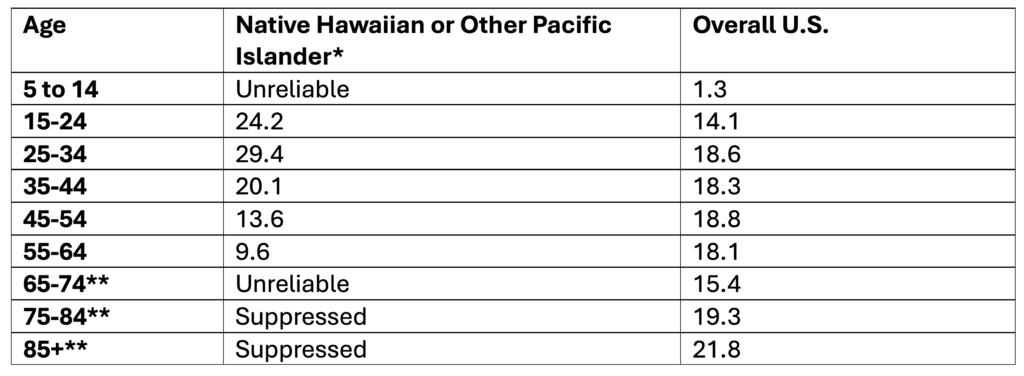
*Non-Hispanic
**Note. Ages 65+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Hispanic or Latino People in the U.S. by Age, 2019-2023
Data Table:
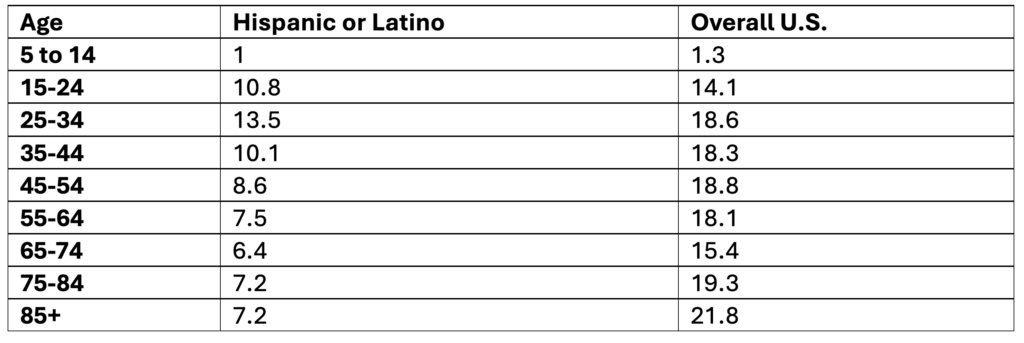
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Hispanic Origin; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Black or African American People by Age, 2019-2023
Data Table:
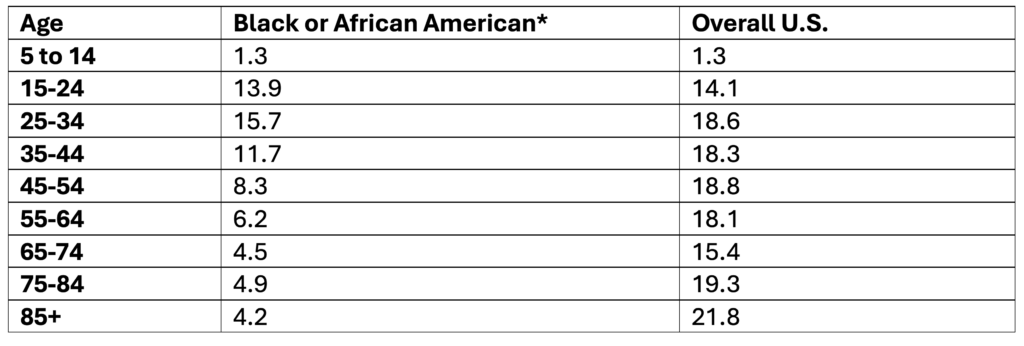
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Asian People in the U.S. by Age, 2019-2023
Data Table:
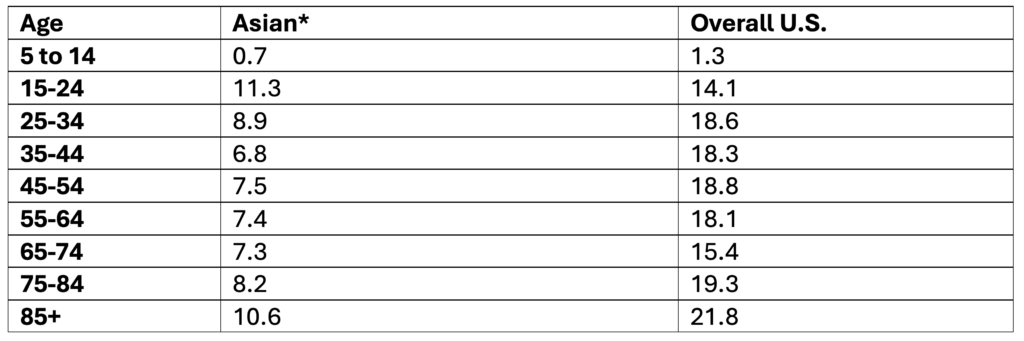
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among American Indian and Alaska Native People by Age, 2019-2023
Data Table:
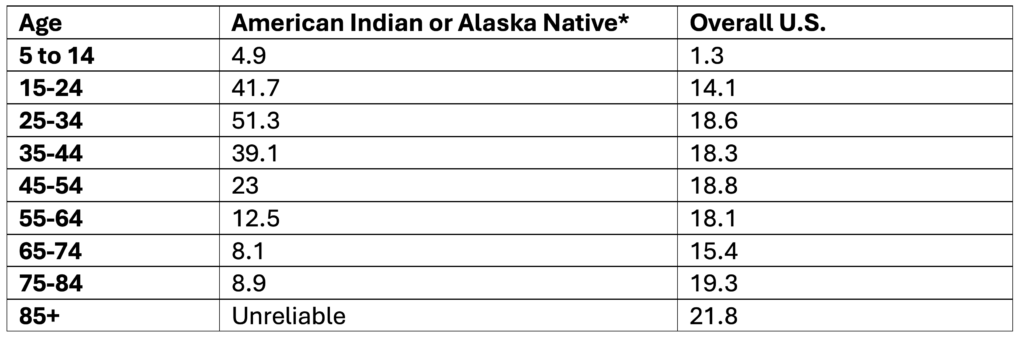
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Past-Year Suicidal Thoughts and Behaviors Among High School Youth, 2023
Data Table:
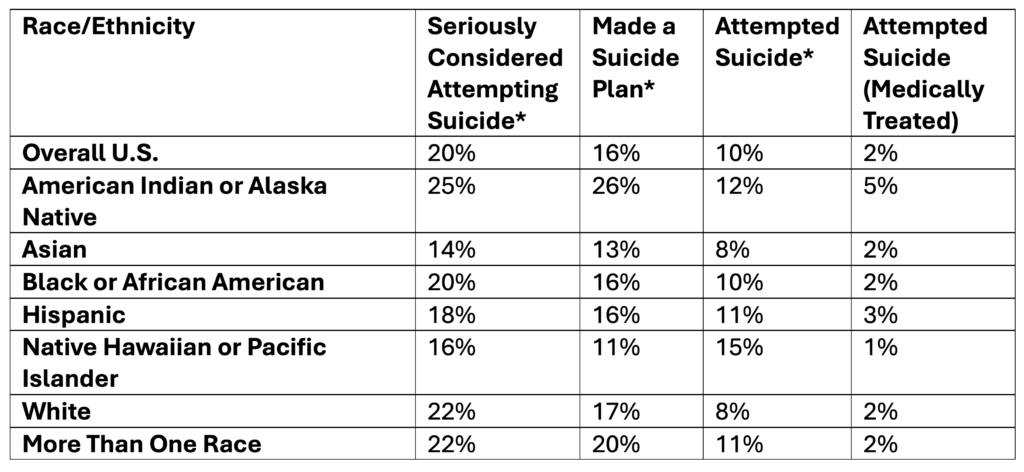
*Self-Reported
Source: CDC, 2025
Citation:
Centers for Disease Control and Prevention (CDC). (2025). 1991-2023 High School Youth Risk Behavior Survey Data. Available at http://yrbs-explorer.services.cdc.gov/.
Past-Year Self-Reported Suicidal Thoughts and Suicide Attempts Among Adults, 2024
Data Table:
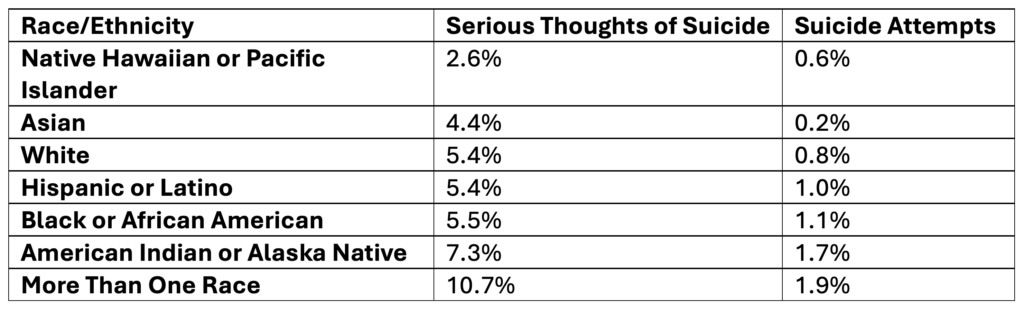
Source: SAMHSA, 2025
Citation:
U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (2025). National Survey on Drug Use and Health 2024 (NSDUH-2024-DS001). Retrieved from https://www.samhsa.gov/data/
Tables: 6.71B & 6.73B
Rates of Suicide by Race/Ethnicity, 2019-2023
Data Table:
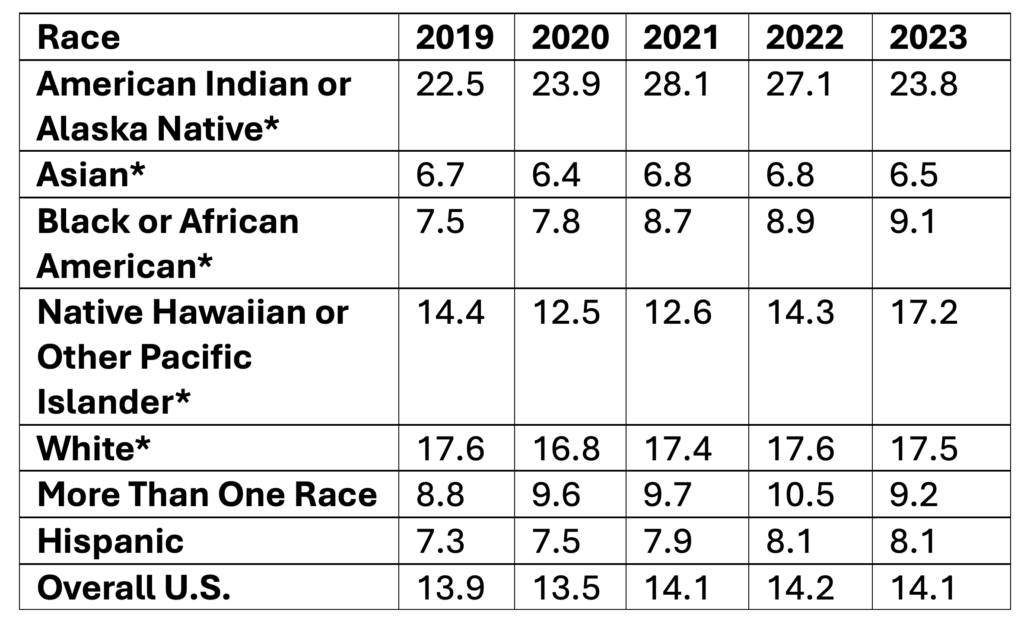
*Non-Hispanic
Age-adjusted rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Single Race 6
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Hispanic Origin
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates by Age, 2019-2023
Data Table:
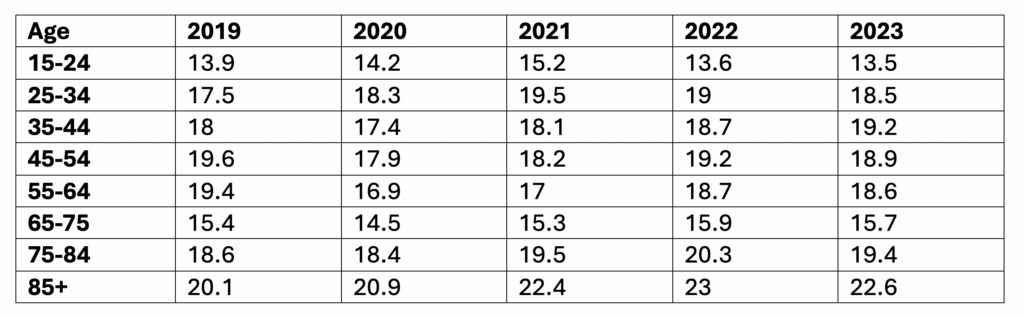
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year, Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)