 Increase Help-Seeking
Increase Help-Seeking
Seeking help for a mental health problem is not easy. Individuals who are struggling with thoughts of suicide or other mental health issues may face any number of barriers.
Barriers To Help-Seeking
- Not recognizing that you need emotional support or professional help
- Not knowing how to find help
- Cultural traditions that value individual independence or frown on seeking help outside of the family
- The mistaken belief that the problems you are facing cannot be resolved, even with assistance
- Lack of access to care, either because of a lack of providers or due to financial issues
The Facts
- Many individuals are affected by mental health problems.
- Mental health issues are not signs of weakness or character flaws.
- Many individuals need help and support to feel better.
- There are many ways to get help and support, including telephone and online sources of assistance, mental health services, peer supports, and other options.
- There are health care professionals who are specially trained to assess suicide risk and provide effective treatment for suicidal thoughts and behaviors.
- There is hope. Individuals with mental health problems can get better, and many recover completely.
Individuals with mental health problems can get better, and many recover completely.
Take Action
- Include people with lived experience on your suicide prevention planning team.
- Identify local and national options for obtaining help, such as the 988 Suicide & Crisis Lifeline, warmlines, online support communities, and mental health services, and promote them through outreach campaigns and other channels.
- Identify and reduce structural and environmental barriers to seeking help. For example, make services more accessible, convenient, and culturally appropriate.
- Educate the community about the warning signs for suicide and correct misinformation.
- When training community gatekeepers to identify and assist people at risk, have course participants identify barriers to seeking help and make plans for how they personally would seek help if they needed it.
- Reduce stereotypes, prejudice, and discrimination by sharing true stories of individuals who sought help and benefited from it.
- Provide information on self-help tools and support options that people can access on their own.
- Train peers to support help-seeking and provide information about available services and resources.
Engaging in strategic planning can help you learn about your community’s beliefs and behaviors about help-seeking as well as available resources, enabling you to focus and tailor your efforts. When promoting help-seeking, it is also essential to plan ahead to ensure that sufficient resources are available to meet an increased demand for services.
Suicide Deaths by Drug Poisoning, 2023
Data Table:

Source: CDC, 2023
Citation:
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]) Available from URL: www.wisqars.cdc.gov
Injury Outcome: Fatal
Injury Type: All Injury
Data Years: 2023
Geography: United States
Intent: Suicide
Mechanism: All Injury
Age: All Ages
Sexes: All Sexes
Race: All Races
Ethnicity: All Ethnicities
Metro/Non-Metro Indicator: None Selected
YPLL Age: 65
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
MCD – ICD-10 Codes: T40.1 (Heroin); T40.0, T40.2, T40.3 (Opium, Methadone, Other opioids); T40.4 (Other synthetic narcotics); T40.5 (Cocaine), T42.4 (Benzodiazepines); T43.6 (Psychostimulants with abuse potential) AND X60-X84 (Intentional sel-harm)
Year/Month: 2023
Group By: Year
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among People of More Than One Race in the U.S. by Age, 2019-2023
Data Table:
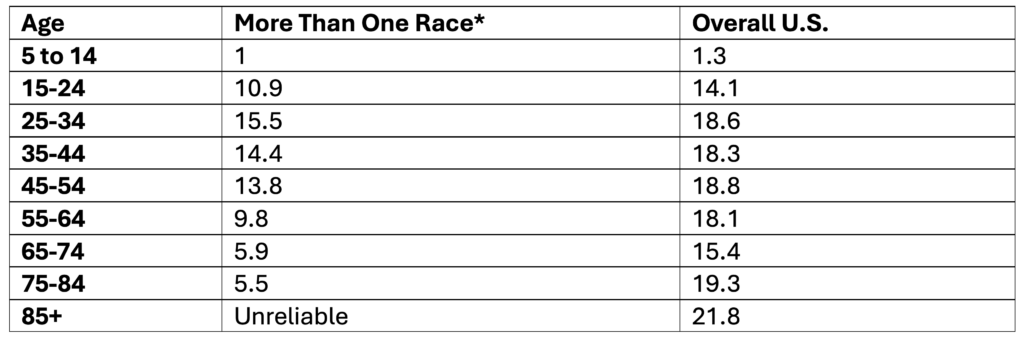
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among White People in the U.S. by Age, 2019-2023
Data Table:
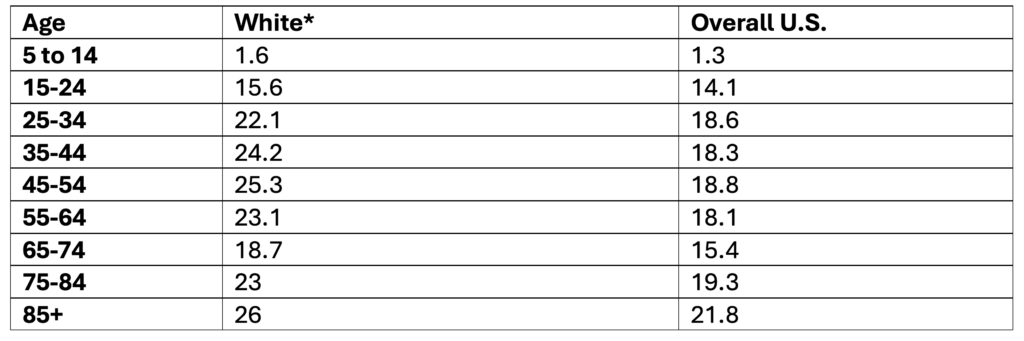
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Native Hawaiian or Other Pacific Islander People by Age, 2019-2023
Data Table:
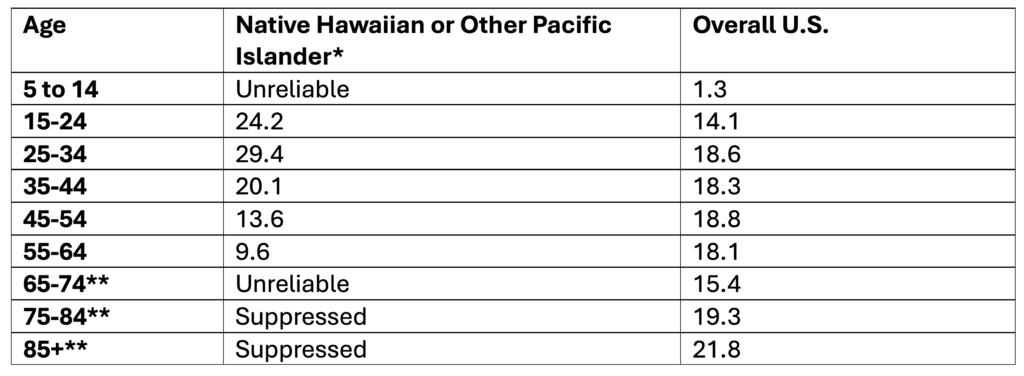
*Non-Hispanic
**Note. Ages 65+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Hispanic or Latino People in the U.S. by Age, 2019-2023
Data Table:
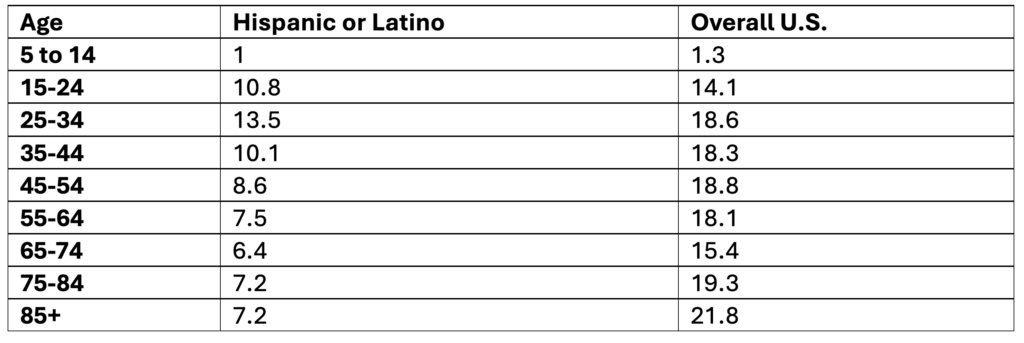
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Hispanic Origin; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Black or African American People by Age, 2019-2023
Data Table:
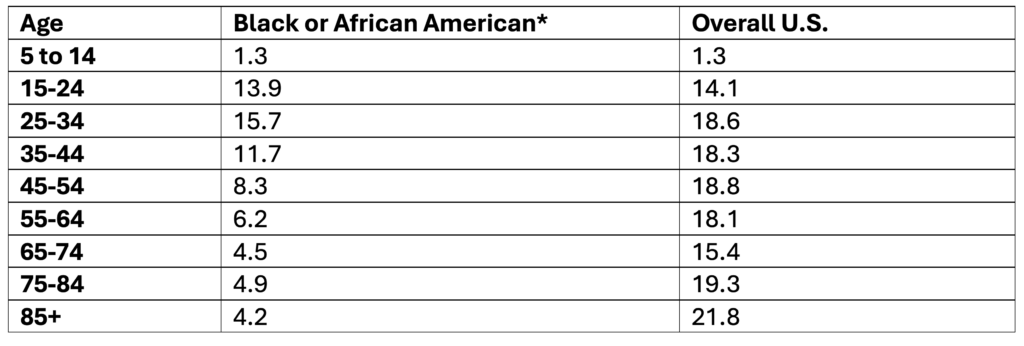
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among Asian People in the U.S. by Age, 2019-2023
Data Table:
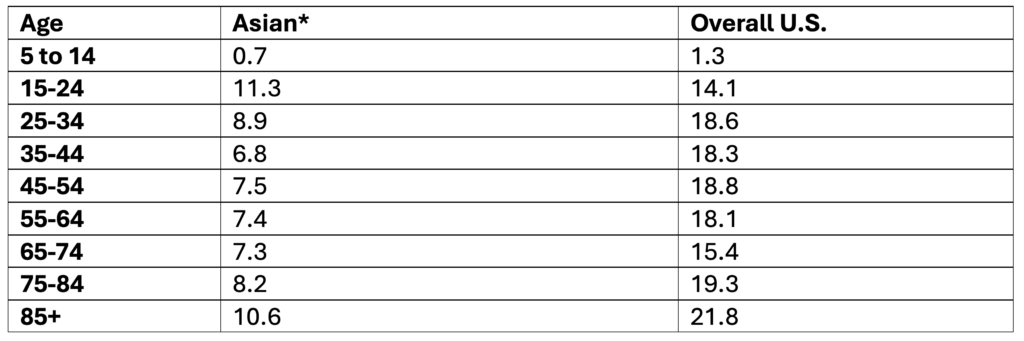
*Non-Hispanic
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates Among American Indian and Alaska Native People by Age, 2019-2023
Data Table:
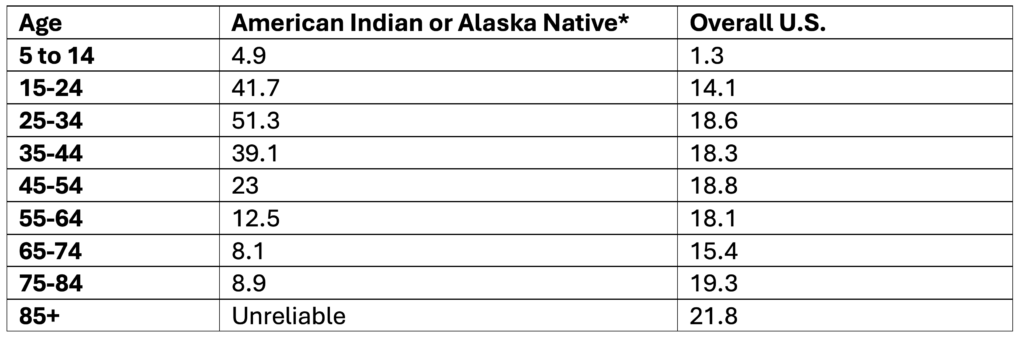
*Non-Hispanic
**Note. Ages 85+ are not reported because data is unreliable
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Single Race 6; Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Ten-Year Age Groups
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Past-Year Suicidal Thoughts and Behaviors Among High School Youth, 2023
Data Table:
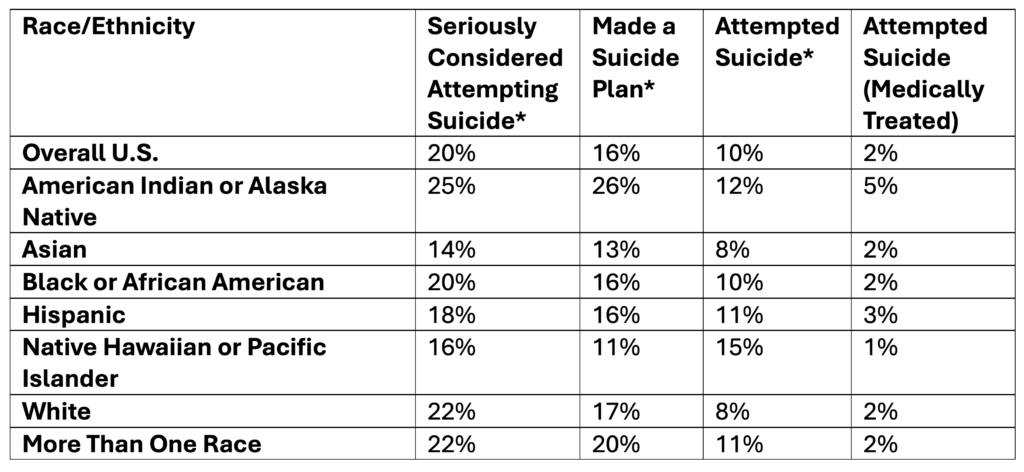
*Self-Reported
Source: CDC, 2025
Citation:
Centers for Disease Control and Prevention (CDC). (2025). 1991-2023 High School Youth Risk Behavior Survey Data. Available at http://yrbs-explorer.services.cdc.gov/.
Past-Year Self-Reported Suicidal Thoughts and Suicide Attempts Among Adults, 2024
Data Table:
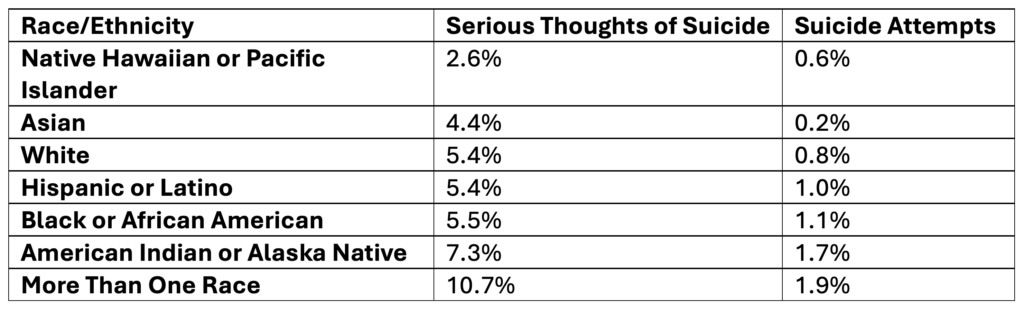
Source: SAMHSA, 2025
Citation:
U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (2025). National Survey on Drug Use and Health 2024 (NSDUH-2024-DS001). Retrieved from https://www.samhsa.gov/data/
Tables: 6.71B & 6.73B
Rates of Suicide by Race/Ethnicity, 2019-2023
Data Table:
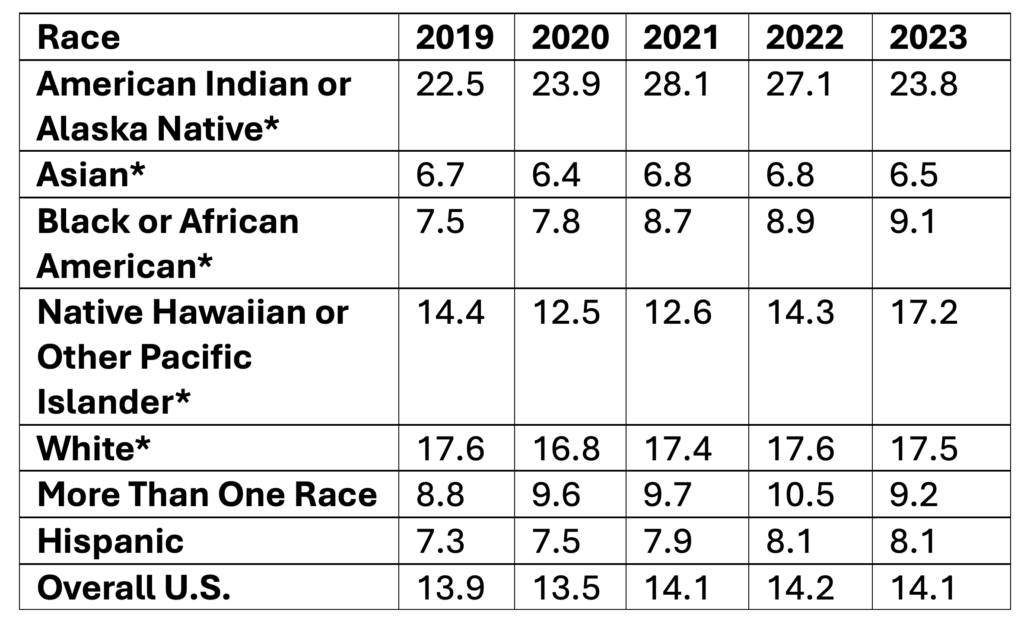
*Non-Hispanic
Age-adjusted rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Hispanic Origin: Not Hispanic or Latino
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Single Race 6
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year; Hispanic Origin
Show Totals: True
Show Zero Values: False
Show Suppressed: False
Standard Population: 2000 U.S. Std. Population
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)
Suicide Rates by Age, 2019-2023
Data Table:
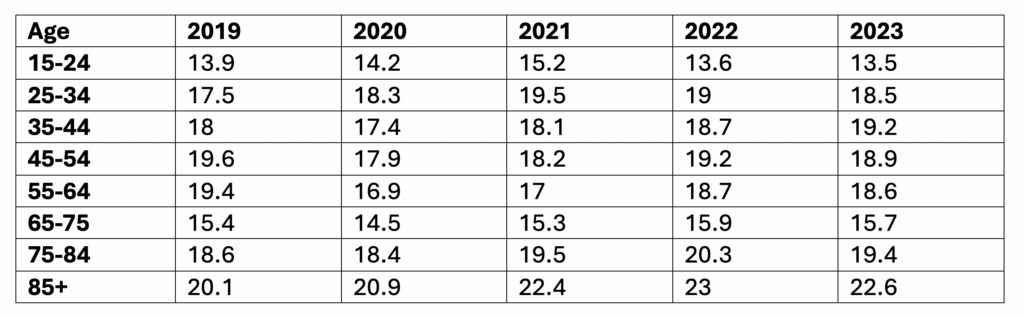
Crude rate per 100,000
Source: CDC, 2024
Citation:
Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 2018-2023 on CDC WONDER Online Database, released in 2024. Data are from the Multiple Cause of Death Files, 2018-2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
ICD-10 Codes: X60-X84 (Intentional self-harm)
Year/Month: 2019; 2020; 2021; 2022; 2023
Group By: Year, Ten-Year Age Groups
Show Totals: Disabled
Show Zero Values: False
Show Suppressed: False
Calculate Rates Per: 100,000
Rate Options: Default intercensal populations for years 2001-2009 (except Infant Age Groups)